Managing the Transition From Inpatient Care
Active handoffs and shared data lead to coordinated care and better outcomes
CCNC’s statewide approach assigns patients a Transitional Care Impactability Score™ to identify those most likely to benefit from an intensive transitional care intervention following a hospital discharge. Targeting this population with specific interventions pays off for patients, providers, and payers.
Preventing Readmissions
Our focus is to create an extremely efficient allocation of care management resources. The key statistic is the “number needed to treat” (NNT) to prevent one inpatient admission in the coming year. For the patient population with a low Transitional Care Impactability Score™, CCNC must intervene with 133 patients to prevent one readmission. However, for the population with a high Transitional Care Impactability Score™, CCNC needs to intervene with only 6 patients to prevent one readmission.
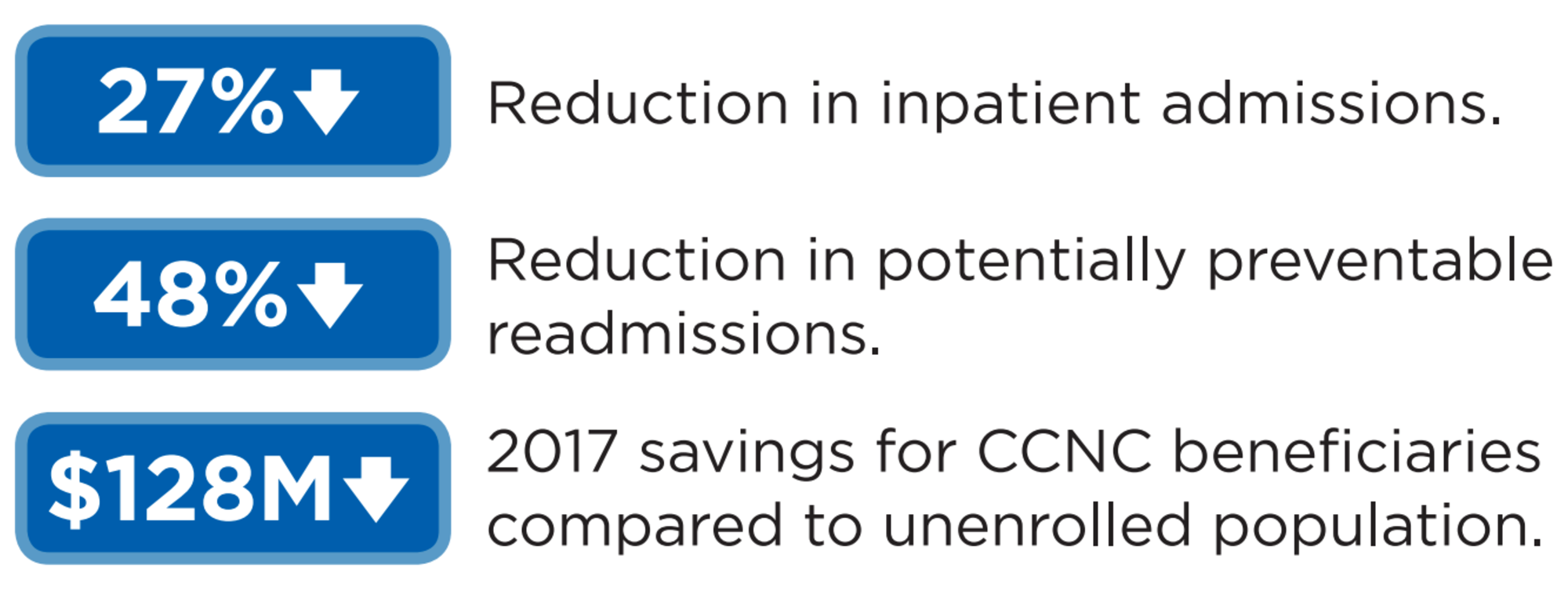
Patients with multiple chronic conditions who receive a CCNC home visit are on average half as likely to have a 30-day readmission compared to those receiving less intense forms of transitional care
Transitional Care Gets Results